When I started my nursing training at Fremantle Hospital 50 years ago in 1965, one of the first things we had to do was go back to school to learn cooking. I couldn’t believe it! We even had the same cooking teacher from John Curtin High School that I thought I had left behind me with the finish of official schooling now that I was working!
Invalid cooking was part of our basic training and meals in hospital were an important part of getting patients better. Nurses were in charge of meals – we didn’t have dieticians. Our Ward Sisters and Staff Nurses trained us in what foods to give each patient – and this depended on their medical condition and to some extent their food preferences were taken into account. And some were very fussy eaters.
I have learnt a lot more since then and there is a lot more research now available. But it is pretty basic really – we eat to supply our bodies with the nutrients needed to sustain a healthy life. If we don’t eat, we die. But before that our health goes down hill.
So we eat to survive and the foods available for us to eat were those that grew or lived around us where we lived. For thousands of years, people lived in the same part of the world and ate the same foods, prepared in traditional ways. This is what we are programmed for. This is what it is easiest for our bodies to deal with. We have developed the ability to digest and use these foods to survive. And the foods around us have developed to survive in the soils and climates they (and we) grow up in too.
This has been the basis for the research I have been involved in with our Polio Clinic and OSWA here in Perth since 1992. The more we investigate this, the more we realise that instinctively we do all really know what we need to eat – BECAUSE IT TASTES GOOD TO US!
We don’t all have the same tastes and our tastes change as the nutrients we need change. That is why we don’t eat the same foods every day for every meal. I have found that people with the same blood groups and same ancestoral backgrounds like the same foods and eat a certain way.
Even in the same family, because we have different blood groups, we can choose to eat with more or less cooking and different things first. One of my sons eats all his veg then all his meat while I must have a piece of meat and some veg with every mouthful. I can’t eat one without the other.
Our research has shown that people who are A or AB blood group don’t usually like legumes ie peas and all sorts of beans, even though they may be eating them believing they are good for them. In fact it has been shown that legumes and lentils can cause clumping of red blood cells resulting in destruction of these useless clumps by the body which thus leads to anaemia. This can happen with other blood groups too but more often in A or AB. I have solved this anaemia in many people by telling them to stop eating legumes. It takes 6-8 weeks to regenerate your red blood cells and so then the GP sees an improvement!
So there is a valid reason behind some natural food likes and dislikes. Babies and animals eat by instinct. They try it and like it or reject it. Most of us have had instinct trained out of us with “Eat everything on your plate!”
Ever wonder why grandma bothered with the long soak, drain, rinse and boil sessions when preparing oatmeal porridge, baked beans and other grains? Or why we are supposed to throw away the water cabbage is cooked in?
There is a good reason that modern research has revealed. Overnight soaking, changing the
water, adding sodium bicarbonate to the water, fermenting, sprouting and cooking – all will alter phytates and decrease or change lectins (or the bad parts of some foods ie with the wrong lock and key) and thus help free up the good nutrients we need.
Our bodies and our foods have and make enzymes that are part of the lock and key effect. The difference in Blood Groups is the slight changes in the surface sugars on all cells, not just red blood cells. It is the complex proteins known as lectins in the foods that can react badly with our body cells. This can change between blood types and food types. The lectin content of foods differ year to year and crop to crop. Climate and soil content affect these changes.
Grains, cereal and legume (especially peanut and soybean) lectins are most commonly associated with reports of digestive complaints. Legumes and seafood have the most abundant sources of lectins in most diets. When lectins affect the gut wall, a broader immune system response may occur as the body’s defenses move in to attack the perceived invaders. Symptoms can include skin rashes, joint pain, leaky gut, sore tummies, bloating, reflux and general inflammation, including allergy-type reactions.
Instinctively we recognise body reactions which we may register as food likes and dislikes as our bodies try to keep us on the right track with the foods we choose to eat. For instance, the summer Valencia orange gives me a tummy ache but the winter Naval orange doesn’t, and tastes better to me. O and AB prefer the taste of the Valencia orange.
I like mulberries when they are red and tangy (a B and A2 blood group preference) while the other blood groups like them when they are ripe and black. Different lock and key.
If we eat foods that naturally appeal to us and taste better, we are more likely to be on the right track. Let each person choose what to put on their own plate ie – help yourself.
This work on lectins is not new. Lectins were first described in 1888 by Stillmark and research on lectins was done by Ehrlich, who was considered to be the Father of Immunology.
If a lectin with a ‘similar’ key comes in contact with one of these ‘locks’ on the gut wall or artery or gland or organ, it can ‘open the lock’, ie ‘break in’, disrupt the membrane, damage the cell and may initiate a cascade of immune and autoimmune events leading to cell death.
Our food likes and dislikes vary with taste, colour, traditional food exposures and blood groups. We should eat the foods of our ancestors – European or Asian, Indian, Chinese. Thai foods are for Thai people! We all have particular enzymes that we inherit and make – that enable us to process and digest safely certain foods but not others eg lactose intolerance, coeliac, nut/eggs allergies.
Compatibility with food types takes thousands of years – we don’t change overnight! Blood types and traditional exposure give key guidelines to what food is suitable to different people. If you don’t have the right key you can’t unlock the door and enter. Each is made to fit the right place/food. Enzymes and co-factors are made in the body from vitamins and minerals and they speed up the digestion of food by enabling chemical reactions, bringing molecules together or pulling them apart. Enzymes lower the amount of energy needed for an action to occur.
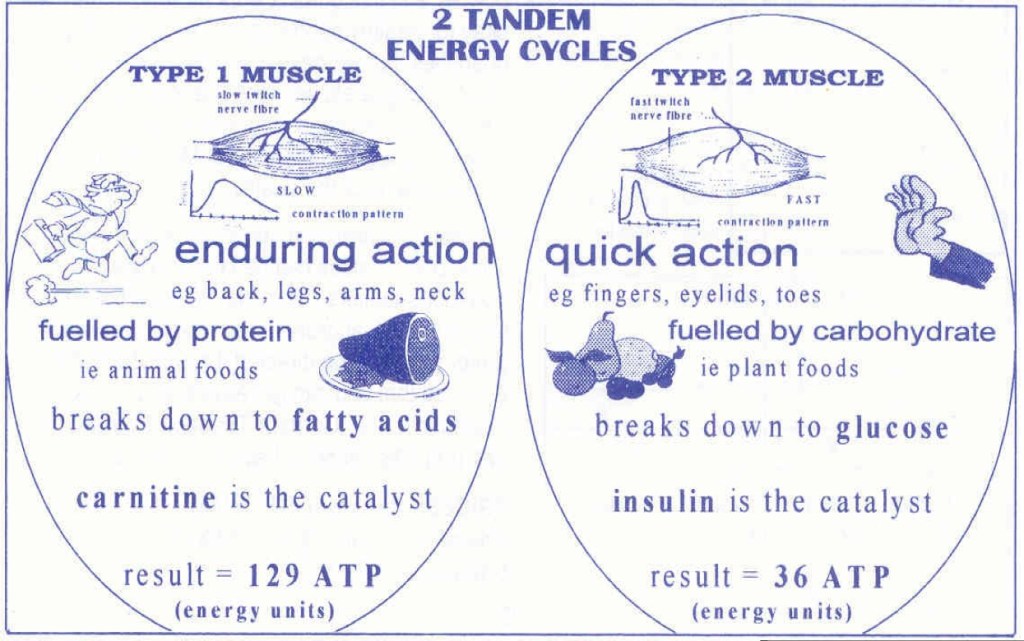
Even the amount of meat – ie protein (animal-based food) to veg – ie carbohydrate (plant-based food) on your plate will vary according to your blood group. Instinctively we will put the right proportions of the right foods onto our plates if we trust our instincts – forget what you have been told or what you have been taught or read is right. Ask yourself what you really want. Remember that cravings may actually be trying to tell you something you are needing and we might have to analyse the truth of them.

O Blood Group – Warm/Hot climate
- Not hungry till 10am -11am
- Picks at food thru day when hungry
- Eats large main meal at night
- Lightly cooked meals eg stir-fry, salads
- Strong digestive system – works while sleeping
- Wakes with energy – ready to go
- Sport activity gets brain going, invigorates
A1 Blood Group – Temperate cool climate
- Hungry when wakes – needs food to warm up eg cooked breakfast, main meal midday
- Light meal at night – digestion poor when asleep
- Long cooked soups and stews, casseroles aid digestion
- Grows grains – rye, barley.
- Ripe fruit but not tropical
- Keeps animals for by-products ie dairy, eggs, wool
- Only eats animals when getting older or bred for food
- Catches fish in rivers and ocean
- Long exercise exhausts, slows brain function
A2 Blood Group – Extreme cold – Arctic
- Scandinavian or Eskimos, Icelanders
- 3 decent meals of meat, fish, root veg
- Strong digestive system
- Need to eat for warmth and energy
- Berries main fruits – some apple, orange, pear, grapes –
- NB stone fruit need frost to set fruit so OK
- No tropical fruits can be grown in Arctic
- No grains grown in snow– may tolerate rye, spelt, rice
- Need lots of protein – meats, fish, fowl, deer, whale, bear
- Long cooked meals – stews, soups, broths
B Blood Group – Cold climate – mountainous
- Developed in Himalayan mountains, spread by gypsies
- Needs 3 reasonable meals – balanced protein and plant foods each meal – get instant reactions to wrong foods
- Need food for warmth and energy
- New-seasons fruit – tangy, not quite ripe
- Cold climate fruit but ok with some warm eg bananas, coconut but not pineapple
- No good with any fowl but eggs ok
- Cold water fish – deep ocean or cold river, no tuna. Salmon ok
- Mountain rice not paddy rice
A1B Blood Group – Warm climate
- Developed in Asia and South Sea islands
- Prefers more vegetables than meat
- Big fish eaters, but not big on chicken or any fowl
- Tropical ripe fruit – oranges ok but not lemon or bananas – good with pineapple but not apple
- Not good with most nuts, dislikes beetroot
- Likes stir-fry, lightly cooked meals
- Instant reactions to wrong foods so may be fussy eater
- Likes potato and root veg, ok with grains
- Avoids legumes esp peas, but eats other greens
- Dislikes stress, usually easy-going, hard workers
A2B Blood Group (very rare) – Cold Climate
- Mostly as for A2 but may need to avoid foods A1B has problems with too eg beetroot, apples.
- Restrictive diet, prone to digestive upsets
- Dislikes stress, usually easy-going, hard workers