The Late Effects of Disability Clinic (LEDC) in WA began in 2000 at the Royal Perth Hospital – Rehab Centre at Shenton Park (where polio was treated 50+ years ago). The pressure that enabled this clinic to be established came from polio survivors in WA, in particular from the Post Polio Network, the local self-help group for polios, in collaboration with some interested health professionals who were already seeing increasing numbers of polios with problems, either privately or through the public hospital system.
It was realised that there were a number of other minority groups also aging with a long term physical disability, like cerebral palsy (CP), spina bifida, Guillain Barre etc, who also needed a voice. By requesting clinical facilities for all of these groups, and pointing out that it is a better use of finances to keep these people out of hospital and still managing at home, we were given a trial run. Health Dept funding was provided for a Rehab specialist to head the clinic for a few hours a week/fortnight, with unpaid physio input from hospital staff as long as it didn’t interfere with their present hospital work commitments. This trial proved its worth and now LEDC has a permanent paid physio employed 3 days per week for the clinic.
Access to LEDC is via GP referral to the Rehab Specialist heading this clinic. The wait time for the doctor is often 9 -12 months, so primary assessment within a few months is undertaken by the physio (Jega) and her team. A helpful exercise regime, tailored to the individual, is set up and monitored, prior to seeing the doctor. Regional video-linked clinics between LEDC and country hospital physio departments for country polios is the next step, along with increased expertise training from the LEDC at Shenton Park to the metro and country community and other hospital, physio departments, who provide on-going care, closer to the homes of polio patients.
This networking by Jega has also been offered to other Australian states and NZ polio groups to assist them to get similar set-ups in their areas. There is further Jega wisdom here.
Main complaints from polios
- fatigue
- weakness
- tripping and falling – more information on balance
- spinal pain (particularly lower back pain) poor balance
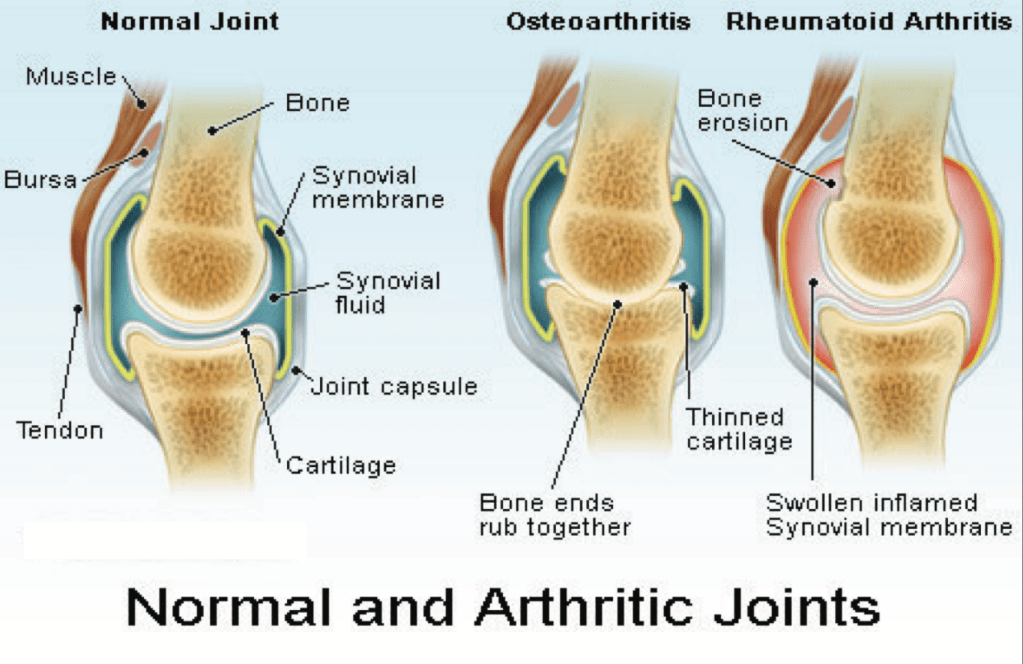
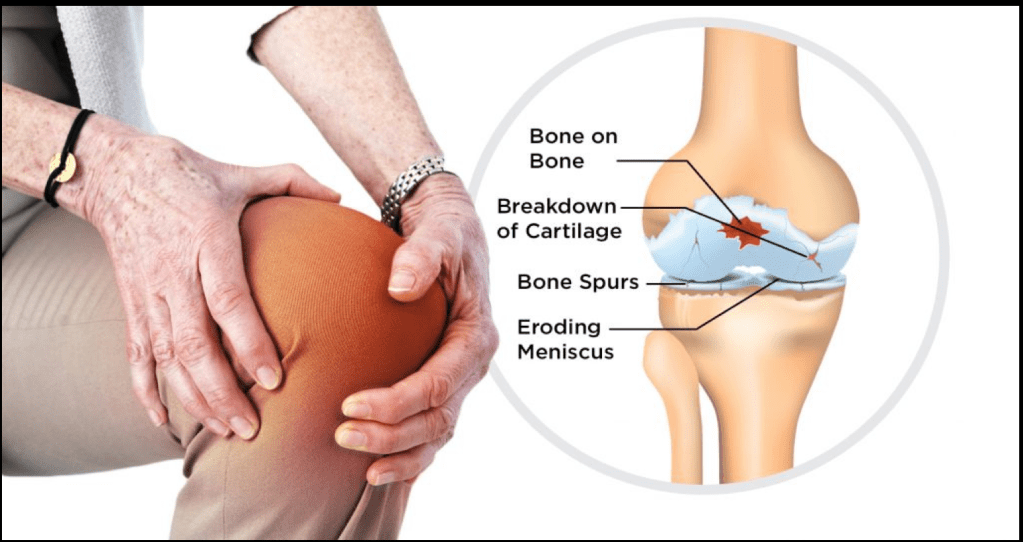
- joint pain
- reduced mobility
- stiffness
- abnormal sensations
- “jumping legs”
- continence issues
- poor sleep
- orthotics devices not working properly
Main findings on assessment
- muscle overuse causing rapid muscle fatigue & increased slower weakness
- loss of muscle units with ageing
- asymmetry of limbs leading to increased pain and reduced function – more liable to osteoarthritis
- disuse weakness – due to age & disability
- substitution of stronger muscles to compensate for weaker muscles
- long-term compensation causing use of weaker muscles more often
- due to poor muscles, polios may be using tightening of ligaments for stability; these have now stretched and are no longer holding limbs in place resulting in hyper-extension eg knees
- polios are having to concentrate on doing all movements, including walking – if distracted, can’t do without conscious thought so more likely to fall
Issues for therapists
- dealing with post polio is complicated; there is a need for therapists with polio experience
- inexperience of GPs, specialists, other physios, OTs, orthotists, podiatrists etc in dealing with polio
- lack of self-confidence in polios themselves – their surprise when changes are made to the way they do things and it actually works!
- differences between testing when standing to testing when walking
- abdominal stability the key to arm and leg use
- solving stiffness problems can actually de-stabilise the patient because of poor muscle bulk (loss of rigidity) thus creating even more problems in body stability to perform actions, prevent falls etc
FOOTWEAR Getting the right shoes are important. Some may need supportive lace-ups, others may need a more flexible shoe to balance better and lessen pain and foot fatigue. The rigidity of the sole of the show can throw you off balance. Watch the weight of the shoe – too heavy for weak muscles.
CALIPERS Off-shelf calipers may not work for polios because of loss of muscle bulk due to polio. Ill-fitting calipers can nerve compression and muscle wastage. The weight of the caliper can become a problem with age and increasing weakness. Regular reviews are necessary as we change over time and getting a “new” one just like the comfortable “old” one is not necessarily going to work.
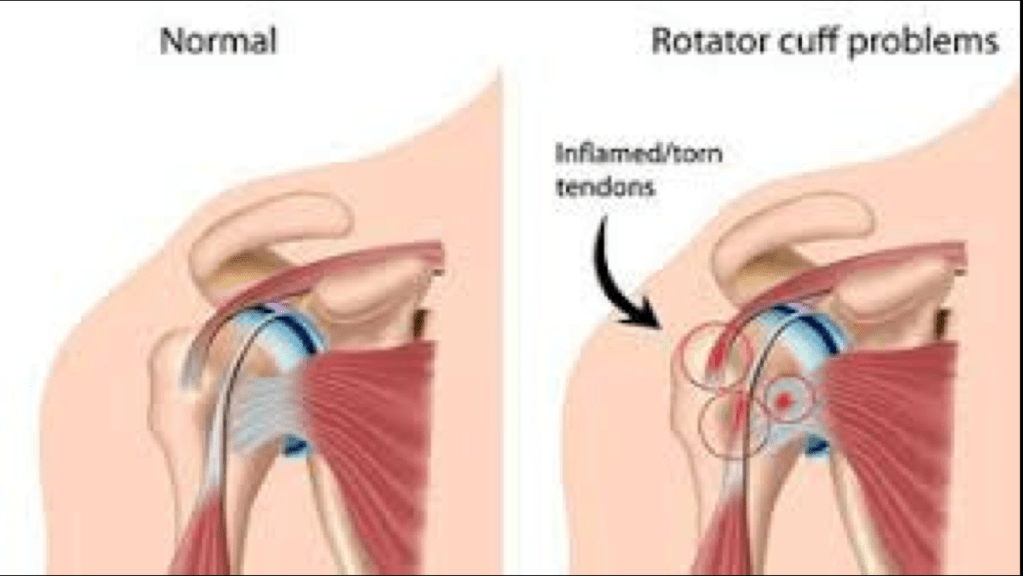
WHEELCHAIRS Seating needs to be carefully measured otherwise it can cause neck and shoulder pain due to poor wheel alignment. Complete assessment of upper limb ability is needed to be sure safe to push wheelchair. Great reluctance to try new types – resistance to change.
WALKING AIDS Seen by polios as sign of failure. Need to be considered earlier as options to conserve strength and energy. Walking sticks can give too much pressure on hand, incorrect height can stress shoulder joint, one-sided support can make more lop-sided, increase stress.
CURRENT ISSUES Need more staff funding. Patients have to travel far for appointments. Lack of allied health professionals. Few health professionals today have any training or expertise with polio anymore. Need to centralise to build excellence & less red tape.
Tips for exercise
Before working out an exercise program I need to know, when and where you had polio. Did you have body, leg or arm weakness? This may have resolved subsequently but may have left you with weakness you are not aware of. If you did have limb or trunk weakness – it will show up as muscles getting tired more quickly in those areas when you use them, particularly as you get older.
Any training can only be done if the muscles are strong enough for the activity. Trunk weakness is a major factor when determining what exercises to do because to pull strong weights, you need strong stomach muscles.
There are 2 types of muscle training – for strength and for stamina. Low weights and high repetitions are essential for stamina. High weights and low repetitions are essential for muscle building and power ie this is speed of movement.
You should train with weights on alternate days and never when you are tired. Try to do weight-training on days when you are not doing other exhausting activities, like sporting-type – swimming, bike, golf or shopping, working etc.
Swimming and bike riding will train for stamina but if the polio leg tires, then it will weaken it, even if the polio limb does not power the movement.
Polio affected limbs are deemed tired, when the quality of your performance starts to fall away, and you are having to think about keeping the limb moving well. It is not when you feel tired.
The key to maintaining independence is conserving your energy so that you can remain independent for longer. Be sensible and use a wheelchair if you need to. Do not let others dictate the speed with which you have to move. Make them push your wheelchair. If it is a manual chair, this will slow them down.
I have supported the use of scooters, so that you can keep up with your social crowd and not wear yourselves out. This way you will still have the energy to walk around the house.
Shopping is another place where a wheelchair or scooter is useful – if only to stop people bumping into you. If you can lean on a trolley and walk and not get tired – this is also a sensible move.
In patients with paralytic polio – “use it or loose it” is only true with qualifications. If you do not do any activity , the limb will get weak. But if you do activity to the point of tiring out the muscle and muscle fatigue sets in, then the limb will also get weak. The key is pacing yourself to your activities. Pacing is going at your own speed; having frequent rest breaks to recover. When quality of movement control starts to falter – stop and recover completely before you continue.
EXERCISE REGIME (suggestions)
- Find the maximum amount of exercise that makes you fatigued and record the time it takes.
- Confine yourself to exercising for only 50% of that time and stop for constant rest periods with several minutes in between. Stop at once if fatiguing.
- Start Day 1 with 5 small sessions spread out over the day. The next time make it 6 repeats, then 7 etc.
- After 3 increases (to 8) then start at 60% with 5 repeats and so on. Stop increasing if you fatigue, go back and work more slowly forward again.